What did local government ever do for us? An update of the evidence.
Levelling up health will only succeed if we invest across the whole of local government.
The Government has committed to levelling up the country and ensuring that no place is left behind. A “levelling up” agenda was introduced to address the longstanding problem of the UK’s economic and social disparities by investing in local infrastructure, empower communities and support economic recovery. Surely, the agenda should also cover a core facet of people’s lives – their health. Indeed, one of the core aims of the agenda is reducing health inequalities across the UK, with an “overarching objective” for improved wellbeing, and the gap across local areas to close. The government has pledged to act on this “unfairness”, and provide opportunities, everywhere, for people to live longer, more fulfilling lives. After all, the health of the people should be the highest law.
There is strong evidence that investment across local government is crucial for levelling up health. This means investment in children’s, housing, cultural, environmental and planning services, as well as in specific public health and social care services. Investment in each of these areas has been cut over the past decade, and cut most in the places where need is greatest, reversing the trend of the previous decade. Whilst this was a disaster for public health even before the pandemic struck, the new cost of living crisis has the potential to greatly exacerbate these trends. The rising cost of living is having a devastating impact on communities, adding to the already devastating impact of the pandemic. Many of the most vulnerable are amongst the least protected from it, and local government services are facing even greater pressure to deliver services for those in need. At this time, what needs to be emphasised is one thing – the importance of investment in local government for public health.
The research outlined here shows how disinvestment in each of these service areas, has come at a cost, damaging the public’s health, leaving still further behind those places where life was already most difficult. It led to increasing infant mortality and a dramatic widening in health inequalities that only worsened during the pandemic.
The message is clear: to reverse this trend, to level up, we need to re-invest across local government; but importantly, we need to invest most in those places with the greatest need. The Levelling Up White Paper prepared by the Government sets out how policy interventions that build on the 2021 Spending Review will deliver change more equally across the UK. Local growth funds, such as the Levelling Up Fund, are meant to provide funding to improve local areas through local projects covering transport, digital connectivity, culture and heritage, and housing. As much of this funding will be delivered through councils, this is an opportunity for the government to put its money where its mouth is and truly level up.
Levelling down – the unequal cuts to local government and stalling life expectancy.
Since 2010, central funding to local government has decreased significantly, leading to a 30% reduction in spending power. Using our most recent data, the overall reduction in adjusted core spending power (i.e. the spending power funded by central government) was over 50% between 2010-11 and 2020-21, the equivalent to £18 billion in real terms. As poorer areas are more reliant on central funding, they are less able to raise income through local taxation. This significant reduction has affected poorer areas the most, where the need for services is greatest. The map below (Figure 1) shows that many of the places that have lost the most are in the North, and this regional variation closely mirrors maps of deprivation and poor health.
Figure 1. Change in local authority spending power between 2010-11 to 2020-21. Values adjusted to 2020 terms using the CPI. Data Source: DCLG.
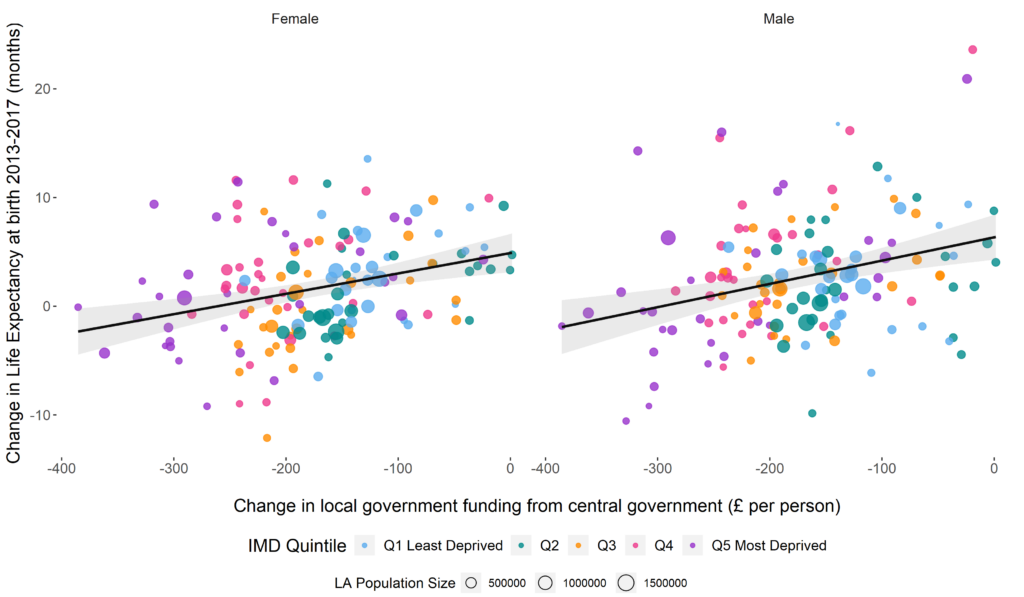
Before the pandemic, it was widely recognised that improvements in life expectancy had stalled over the last decade and inequalities were widening. Our analysis shows how cuts to local government funding made a significant contribution to these adverse trends in mortality. Over a 5-year period, these cuts led to an estimated 10,000 additional deaths in England, in people under 75 years of age, compared to what would have been the case if local government funding had not been cut. As funding was cut more in the most deprived local authorities, the effect on mortality was greater in those areas, widening the already stark health inequalities (see figure 2).
Figure 2. Association between change in central government transfers to each local authority area and change in life expectancy for men and women between 2013 and 2017.
Other studies have demonstrated that austerity measures and cuts to LA budgets have impacted upon many health outcomes, supporting the idea that cuts to local authority budget had, unsurprisingly, significant health impacts. For instance, the decline in service spending was associated with increased hospital admissions for nutritional anaemia. In line with austerity-related reductions, increased admissions were not evenly distributed across the country, with greater impacts in more deprived areas. Similarly, other studies have shown how the local fiscal austerity over the last decade was associated with worse multimorbidity and health-related quality of life. It is likely that those who might not have the income to seek out private services, and those who already have a chronic condition and generally higher public service need, are most likely to be worse affected by these spending cuts.
With such financial constraints, councils had no other option than to cut back on the services they delivered. But what services have councils been forced to cut? These cuts were not evenly distributed among service areas. In general, because councils have statutory responsibilities to provide some services – such as adult and children’s social care – they have maintained funding for these, whilst cutting discretionary services, including transport, housing, leisure, environmental, cultural and planning services (see figure 3). These are important services that tackle the root causes of health inequalities.
Figure 3. Trends in spending per person by service line in England between 2004-05 to 2020-21.
While there has been a substantial increase in spending in 2020-21, this is potentially driven by the emergency funding given to Local Authorities during the pandemic. In 2020-21, the government has provided additional funding through the COVID-19 2020/21 Emergency Unringfenced Funding (4 tranches), the Sales, Fees and Charges Compensation Scheme, and the COVID-19 Business Rates Reliefs, for a total of £11.96 billion – equivalent to approximately 10% of their total service expenditure.
Investing in the best start in life.
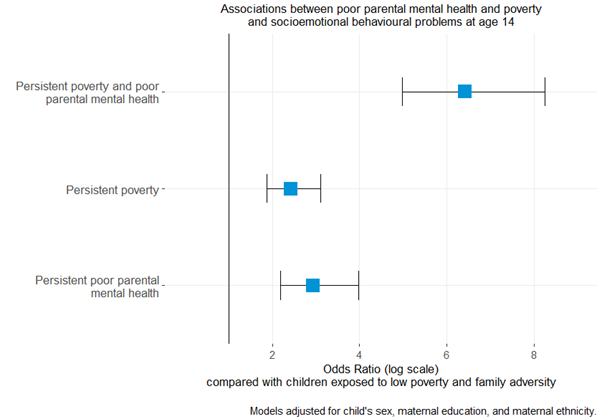
In a recent study we assessed the impact on children’s health of childhood adversities that cluster with poverty. Persistent poverty or persistent poor parental mental health affects over 40% of children in the UK. The combination of both affects one in ten children and is strongly associated with adverse child outcomes – these children are many times more likely to experience socioemotional issues compared to those in more affluent families (figure 4). Subsequent analysis showed that these combined exposures explain about half of the burden of mental health problems in adolescence.
While these harmful exposures are very common in England, they are much more prevalent in Northern regions compared to the Southern regions (55% compared to 32% respectively). The “Child of the North” report further illustrates how children in the North are more likely to live in poverty than those in the rest of England, leading to worse physical and mental health outcomes, and widening the already stark inequalities present.
Figure 4. Associations between poor parental mental health and poverty, and socioemotional behavioural problems at age 14. Source: Adjei, N. K. et al. (2021).
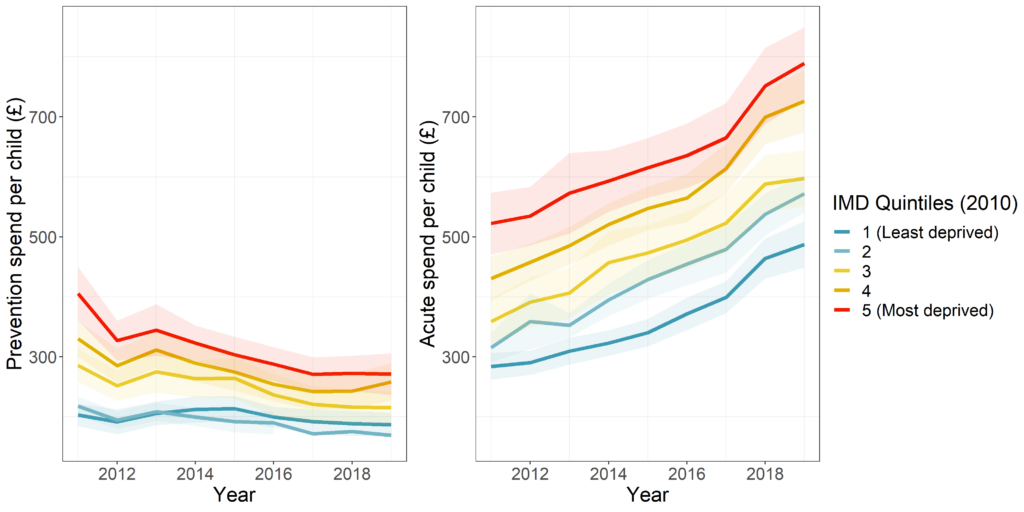
Multiple reviews have highlighted that one of the most cost effective approaches to reducing health inequalities is to invest in children. One might think from figure 3 above that spending on children’s services has been relatively protected from a decade of austerity. But this is very far from the truth. In fact, there has been continuous disinvestment in the very services that Sir Michael Marmot, in his 2010 review of health inequalities, recommended investing in – giving every child the best start in life. Local government spending on preventative early years and youth services (including Sure Start) fell by 21% over the past decade, these declines being greatest in the most deprived areas (see figure 5).
Overall spending on children’s services increased because of a massive rise in the number of children being taken into the care of the local authority – spending on this increased by 68%. Being taken into care as a child is a marker of severe deprivation, and those children tend to go on to face adversity throughout their lives. We have increased the cost of pulling drowning people from the river, whilst disinvesting in the services that prevent them from falling in, in the first place.
Figure 5. Trends in local authority spend on prevention services for children and young people and spend on safeguarding and children taken into care, by deprivation level in England.
Our research has shown that these increases in children being taken into care have been greatest in the most deprived areas, the very places where preventative services have been most severely cut. We estimate that between 2015 and 2020, over 10,000 children under the age of 16 entering care were linked to rising child poverty.
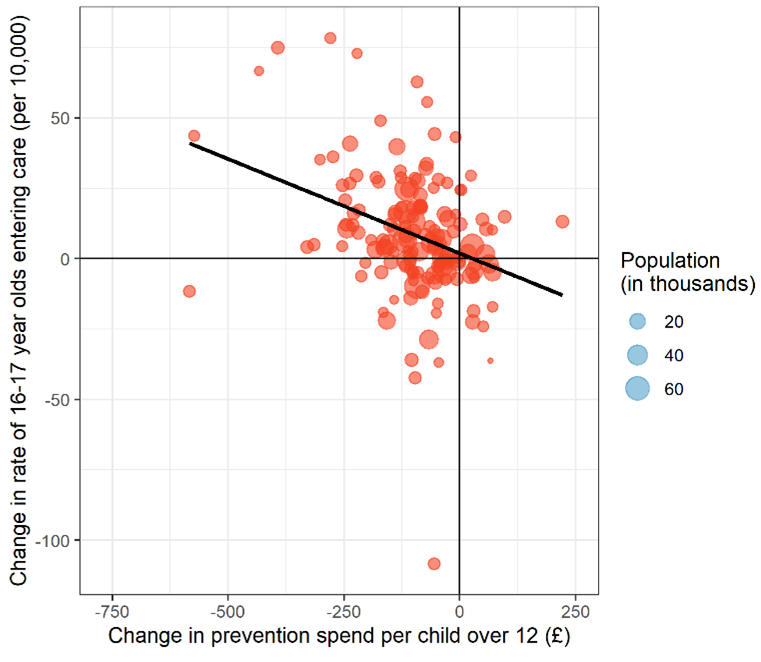
A further study of ours has shown that reductions in spending on preventative services for adolescents is directly linked to rising rates of 16 and 17-year-olds entering care (see figure 6). Every £10 decrease in prevention spend per child was associated with an estimated additional two 16-17 year old children entering care per 100,000 per year. In total, we estimate that an additional 1,000 children aged 16-17 were taken into care, over 8 years, than would otherwise have been expected had 2011 levels of prevention spend been sustained. This added an extra £60 million to councils’ care bills, wiping out any savings from cutting prevention spend. If these cuts in prevention services are not reversed, they will contribute to spiralling costs in the future.
Figure 6. Associations between changes in local authority prevention spend on adolescents and changes in adolescents entering local authority care, between 2011 and 2018.
The positive effect of prevention, and the negative impact of reducing prevention is clear. This is particularly the case for early years services, such as Sure Start children’s centres. Local authority-run children’s centres have been an important source of community-based support for children aged under 5 and their families, including not only parenting programmes but links with employment and welfare support for parents, especially in more deprived communities. Children’s centres have been one of the successes of government policy in the UK, providing joined up support for parents and children when they need it most. A study by the institute for Fiscal studies (IFS) has shown that investment in Sure Start reduced hospital admissions during childhood, especially for children living in the most deprived neighbourhoods. But cuts to preventative children’s services outlined above have led to the closure of many Sure Start centres. Evidence of the adverse consequences of this decision, is now emerging.
In our recent study, we show that cuts in spending on Sure Start has contributed to an increase in childhood obesity. We estimate that several thousand additional children became overweight or obese compared with the expected number if spending levels had remained at 2010 levels. Reinvesting in Sure Start should be part of the government’s strategy to reduce childhood obesity. These cuts are likely to have also contributed to the recent widening of the obesity gap between the least and most deprived children. Cuts to spending on Sure Start have also been linked to worse child development as children start school.
Sure Start’s impacts on child health last well beyond the end of the programme – some of the biggest impacts are felt well into adolescence. But deprived communities have worse access to good-quality children’s services. An analysis of inspection outcomes by Ofsted on local authority children’s services suggests that both greater expenditure on preventative children’s services and lower levels of deprivation are associated with higher likelihoods of a positive quality inspection outcomes. Each £100 increase in preventative spending per child was associated with a 69% increase in the odds of a positive Ofsted inspection. An inverse care law can have wider implications on how funding for children’s services is distributed. Ofsted outcomes are not simply meaningless assessments of quality: “inadequate” judgements could result in said services being restructured or removed from public control under a pretence of quality improvement – despite evidence that disinvestment in services and exacerbated poverty are the root cause for these outcomes.
The health impact of local government housing services.
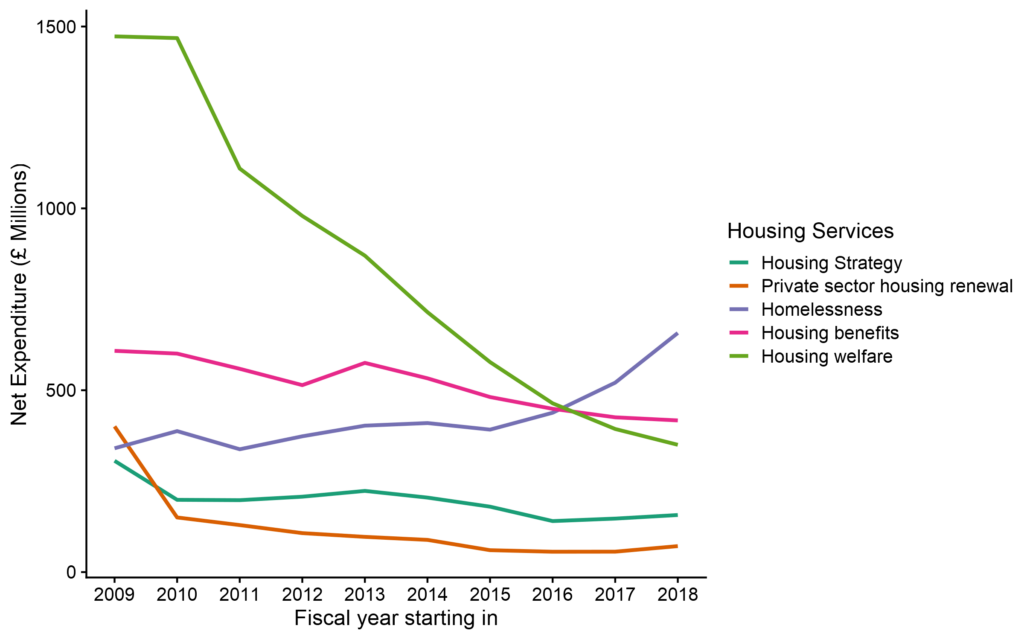
The link between housing and health has long been recognised. Whilst local governments are less involved than they use to be, in the direct provision of council housing, they continue to provide critical housing support services – including temporary accommodation, housing advice, homelessness prevention, rent rebates and housing welfare. Housing is one of the areas of local government that has experienced the most severe cuts. Spending on housing services and homelessness prevention declined by over 50% in between 2009 and 2019.
Our analysis shows that these cuts have particularly affected housing welfare services, such as the Supporting People Program (figure 7). These programs provide housing support for vulnerable groups, such as people with poor mental health, women at risk of domestic violence, young people leaving care, or people with drug or alcohol use problems.
As we saw with children’s services, alongside these cuts in prevention we have seen increases in spending on acute adverse events. Spending on homelessness, including temporary accommodation, has seen a significant rise, particularly in more recent years. The consequences and costs of the disinvestment in prevention has been severe. Street homelessness has been rising steadily, with numbers doubling between 2013 and 2018, and this has led to increased number of homeless people dying. Homelessness and substance misuse are often linked, and drug deaths have been rising steadily over the last decade, reaching record levels in 2020.
Figure 7. Trends in spending on local government housing services in England. Data source: MCHLG.
In a recent study, we showed that reductions in funding for housing services were associated with increased deaths from drug misuse, accounting for an additional 1000 deaths from drug misuse between 2013 and 2018, 7% of all drug-related deaths during that period. It is likely that local government’s inability to secure the appropriate accommodation for homeless individuals and households, and inadequate preventative, advisory and supportive services for vulnerable groups, has contributed to the recent increases in drug deaths.
While rising homelessness is a critical issue, there are also wider challenges around housing affordability and quality. There is significant evidence of how unequal distribution of poor-quality homes across the population correlates with other social inequalities in health; and the current cost-of-living crisis may exacerbate the issue. This is particularly the case within the private rented sector: since the early 2000s, the private rented sector doubled, in tandem with falling housing affordability and a decline in the social housing sector. While local authorities gained discretionary powers to regulate privately rented homes through “selective licensing” since 2006, the effects of these schemes have not been properly explored. A recent study has found links between said interventions and improved mental health outcomes in London, as well as reduced anti-social behaviour at the area level. However, more research is needed to examine these effects in more detail and across England.
The environment in which we live.
Local government is central to so much that makes places good places to live. Councils are the biggest investor in sport, leisure, parks, and green spaces, spending £1.1 billion per year in England. Providing opportunities for physical activity that are affordable for all is crucial for addressing health inequalities. Local authority sport and leisure facilities play an essential role in giving children the best start in life, with 72% of schools relying on public swimming pools to teach children how to swim. Our previous research has shown that by reducing the cost of using leisure facilities, local authorities can have a major impact on levels of physical activity – and importantly, increase the physical activity of more disadvantaged groups who have previously been the most inactive.
The urban green spaces, such as parks, playgrounds, and residential greenery, that local governments develop and maintain, can promote mental and physical health, and reduce morbidity and mortality. Local council libraries, museums and art galleries have also been shown to improve social cohesion, as well as providing educational opportunities, developing digital skills, assisting with job applications, and increasing employability. Environmental and regulatory services provided by local government also play a vital role in public health. These services help manage environmental health hazards, such as air and noise pollution, infectious diseases, and regulating industries. Further, local government’s planning and developmental services are responsible for community and economic development plans that influence local jobs, transport and living environments, all of which have important implications for health.
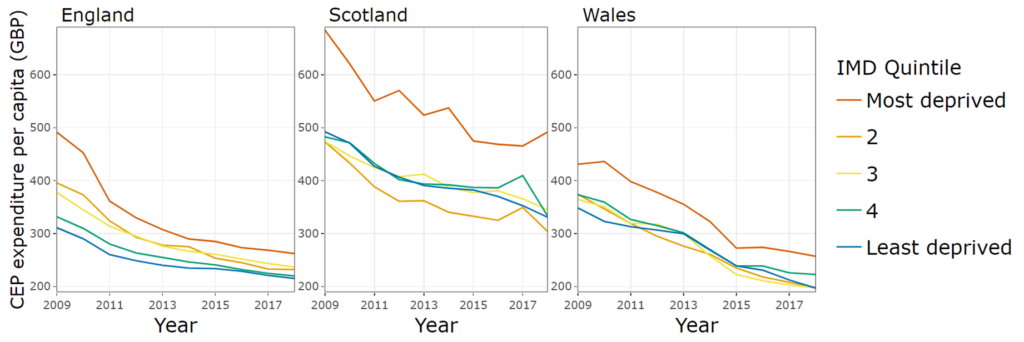
These Cultural, Environmental and Planning (CEP) services have also been cut by 50% during the last decade. Our research suggests that whilst similar cuts have taken places across the countries of the UK, it is only in England that these have been regressive, reducing funding most in the most deprived areas (see figure 8). However, it is difficult to assess the health impact of such services; the health effects of CEP may well be dwarfed by the effects of spending on larger budget lines such as education, children’s services and social care. More importantly, CEP services offer a wide range of services, and finer scales may be required to detect their influence on health outcomes, such as obesity in children.
Figure 8. Gross expenditure per capita on Cultural, Environmental and Planning services by country and level of deprivation.
What is to be done?
The evidence is clear. Investment across local government reaps public health benefits and disinvestment causes harm. This is not just about investment in specific “public health” services provided by local government such as smoking session, sexual health or drug and alcohol services, although these have also been cut by £1 billion (even though investment in these services leads to greater benefits than investment in the NHS). Investment across the whole of local government is needed to level up health, including investment in housing, children’s, leisure, cultural, environmental, and planning services.
The government has committed to levelling up health and ensuring everyone has the chance to live happy and healthy lives. Boris Johnson called the widening differences in life expectancy between places an outrage. His predecessor, Theresa May, in her first speech as prime minister vowed to fight against this burning injustice. Unfortunately, under the stewardship of the past three prime ministers this health divide has increased, reversing the trend of the previous decade. The pandemic has led to a further dramatic deterioration in health equality, hitting the poorest places hardest, increasing the need for urgent action.
The evidence we present here shows that these differences in health can be reversed by getting the right resources to the places that need them most. The upcoming spending review is the opportunity to do that, by investing in the conditions needed for a healthy life – investing in local government. Achieving the government’s ambition will require a reversal of the cuts to local government, but we also need to ensure resources are shared between places in proportion to their needs.
The UK Government has declared that austerity is over and has committed to investing more to support places that have previously been left behind. This commitment has become increasingly important following the COVID-19 pandemic. It’s time to move beyond rhetoric to ensure fair investment in local government to level up health. The wider “levelling up agenda”, has already received criticism regarding the competitive mechanisms with which local growth funds are allocated to places. It is crucial that not only are funds distributed in a manner that allow for equitable recovery, but also in assessing the relative need of each Council, the drivers of poor health are considered across all areas of local government services.
Further reading
Alexiou A, Fahy K, Mason K, Bennett DL, Brown H, Bambra C, Taylor-Robinson D, Barr B. Local government funding and life expectancy in England: a longitudinal ecological study. The Lancet Public Health 2021; 6: e641–7. https://doi.org/10.1016/S2468-2667(21)00110-9.
Jenkins, R, Vamos, EP, Mason, K. et al. Local area public sector spending and nutritional anaemia hospital admissions in England: a longitudinal ecological study. BMJ open, 2022; 12(9), e059739. https://doi.org/10.1136/bmjopen-2021-059739.
Adjei, NK, Schlüter DK, Straatmann, V, et al. Impact of poverty and family adversity on adolescent health: a multi-trajectory analysis using the UK Millennium Cohort Study. The Lancet regional health. Europe. 2021; 13:100279. https://doi.org/10.1016/j.lanepe.2021.100279.
Bennett DL, Schlüter DK, Melis G, et al. Child poverty and children entering care in England, 2015–20: a longitudinal ecological study at the local area level. Lancet Public Health. 2022; 7: e496-e503. https://doi.org/10.1016/S2468-2667(22)00065-2.
Bennett DL, Mason K, Schlüter DK, Wickham S, Lai ETC, Alexiou A, Barr B, Taylor-Robinson D. Trends in inequalities in Children Looked After in England between 2004 and 2019: a local area ecological analysis. BMJ Open 2020;10:e041774. http://dx.doi.org/10.1136/bmjopen-2020-041774.
Bennett DL, Webb CJR, Mason K, Schlüter DK, Fahy K, Alexiou A, Wickham S, Barr B, Taylor-Robinson D. (2021). Funding for preventative Children’s Services and rates of children becoming looked after: A natural experiment using longitudinal area-level data in England. Children and Youth Services Review, 131, 106289. https://doi.org/10.1016/j.childyouth.2021.106289.
Higgerson J, Halliday E, Ortiz-Nunez A, Brown R, Barr B. Impact of Free Access to Leisure Facilities and Community Outreach on Inequalities in Physical Activity: A Quasi-Experimental Study. Journal of Epidemiology and Community Health, 12 January 2018, jech-2017-209882. https://doi.org/10.1136/jech-2017-209882.
Higgerson J, Halliday E, Ortiz-Nunez, A, Barr B. The Impact of Free Access to Swimming Pools on Children’s Participation in Swimming. A Comparative Regression Discontinuity Study. Journal of Public Health, 2018. https://doi.org/10.1093/pubmed/fdy079.
Mason K, Alexiou A, Bennett DL, Summerbell C, Barr B, Taylor-Robinson D. Impact of cuts to local government spending on Sure Start children’s centres on childhood obesity in England: a longitudinal ecological study. Journal of Epidemiology and Community Health 2021;75:860-866. http://dx.doi.org/10.1136/jech-2020-216064.
Webb, C., Bennett, D., & Bywaters, P. Austerity, Poverty, and Children’s Services Quality in England: Consequences for Child Welfare and Public Services. Social Policy and Society, 1011; 1-22. Doi:10.1017/S147474642200001X.
Alexiou A, Mason K, Fahy K, Taylor-Robinson D and Barr B. Assessing the impact of funding cuts to local housing services on drug and alcohol related mortality: A longitudinal analysis using area-level data in England. International Journal of Housing Policy, 2021. https://doi.org/10.1080/19491247.2021.2002660.
Petersen J, Alexiou A, Brewerton D, et al. Impact of selective licensing schemes for private rental housing on mental health and social outcomes in Greater London, England: a natural experiment study. BMJ Open 2022;12:e065747. doi: 10.1136/bmjopen-2022-065747.
Barr B, Alexiou A, Bennet DL, et al. The impact of contrasting investment strategies at the local level. February 2021. Available at: https://sphr.nihr.ac.uk/research/places-communities/quantifying-and-evaluating-the-impact-of-contrasting-investment-strategies-at-the-local-level-wsa-wp2/ (unpublished analysis).
Fahy K, Alexiou A, Mason, K et al. Inequalities in local government spending on cultural, environmental and planning services: a time-trend analysis in England, Scotland, and Wales. BMC Public Health 23, 408 (2023). https://doi.org/10.1186/s12889-023-15179-9.
Mason K, Alexiou A, Barr B, Taylor-Robinson D. Impact of cuts to local authority spending on cultural, environmental and planning services on inequalities in childhood obesity in England: A longitudinal ecological study. Health & Place 2023; 80: 102999. https://doi.org/10.1016/j.healthplace.2023.102999.
Funding
This research was funded by the National Institute for Health Research School of Public Health Research (NIHR SPHR) and the NIHR Applied Research Collaboration Northwest Coast (NWC ARC). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health and Social Care or Public Health England.